



Hi! - ENG





Our commitment to the patient is to be able to compensate for the loss of hard and soft tissue so that 3D positioning of the implant is correct, the hygiene and esthetics of the implant-supported crown is optimal and the reliability of our treatment is not compromised in the long term.
The current esthetic demands presented by many patients have led to updating success criteria in dental implants in the anterior region and now involve not only osseointegration of the implant, but also the long-term peri-implant stability of hard and soft tissue.
This peri-implant stability may be compromised when there is already tissue loss resulting from the inevitable remodeling of post-extraction sockets. It is for this reason that when dealing with the anterior region, we have to view therapeutic options that can help us to reduce or compensate the inevitable remodeling of the post-extraction socket by means of alveolar regeneration or immediate implant dentistry.
Our commitment to the patient is to be able to compensate for the loss of hard and soft tissue so that 3D positioning of the implant is correct, the hygiene and esthetics of the implant-supported crown is optimal and the reliability of our treatment is not compromised in the long term.1
The role played today by immediate implant dentistry and immediate loading in the anterior region2, 3 is of paramount importance in order to understand that any surgical procedure to position an immediate implant implies correct management of the socket, mucosa and design of the provisional prosthesis until obtaining the final crown.4, 5, 6
We are therefore faced with what is known as a “surgery-periodontology-prosthetic balance”, in which the three specialties will be responsible for providing us with a reliable long-term result when dealing with the anterior esthetic region.
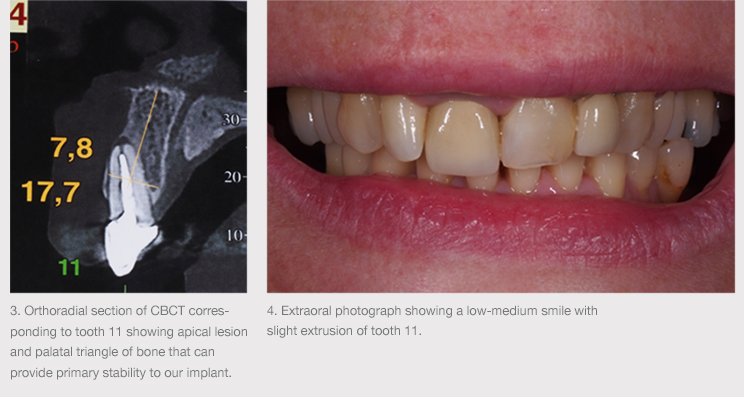
Below is a clinical case of coronal fracture of tooth 11 with periapical lesion showing tooth extraction. Two treatment options were here taken into account:
Option 1: Tooth extraction with alveolar regeneration and deferred implant positioning
Option 2: Tooth extraction with immediate implant positioning
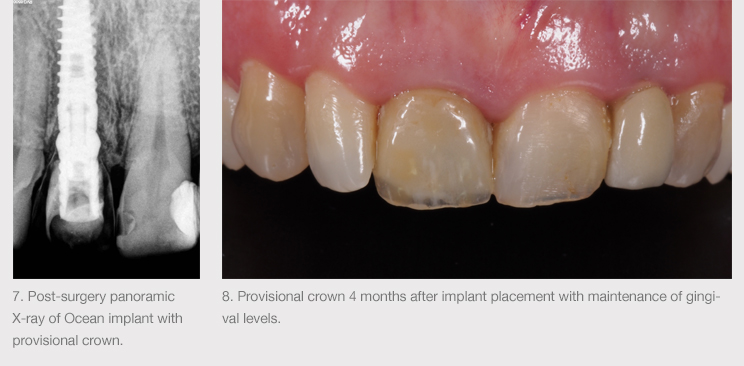
Following clinical, radiographic and tomographic examinations, it was decided to proceed with the extraction of tooth 11, immediate implant and immediate esthetic loading in order to be able to control and compensate for bone and soft tissue remodeling of the post-extraction area.1
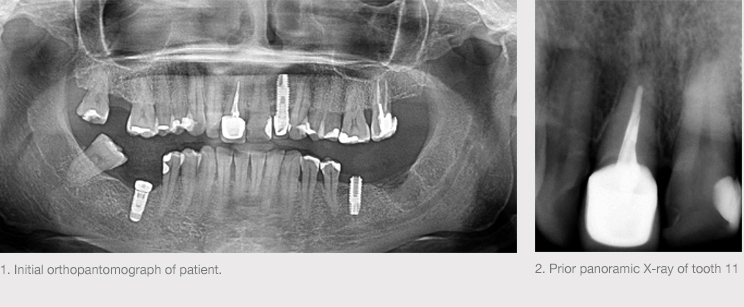

Tooth 11 was extracted and an Avinent Implant System Biomimetic Ocean (3.5 x 13 mm) implant was positioned, prosthetically guided by a surgical guide made of resin that provided correct 3D positioning of the tooth to be restored and would simultaneously serve as an immediate loading provisional crown.

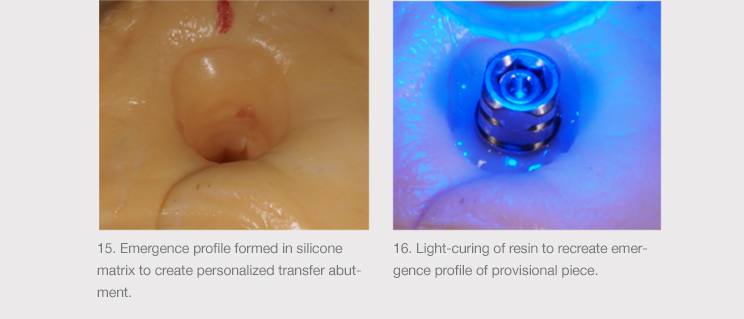
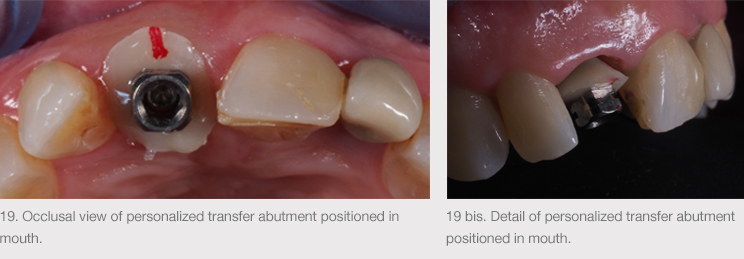
Insertion torque was 45 Ncm, the implant holder was removed and the implant was grinded to be able to line it with the provisional crown of the surgical guide. Following the critical and subcritical contour guidelines established by Óscar González,7 the provisional crown was screwed on and the implant holder was lined, previously having been painted with opaque so that the provisional crown could be left for a total of 4 months, thereby adequately handling the mucosal contour. After the third month of loading, the emergence profile was modified to obtain the current mucosal level.


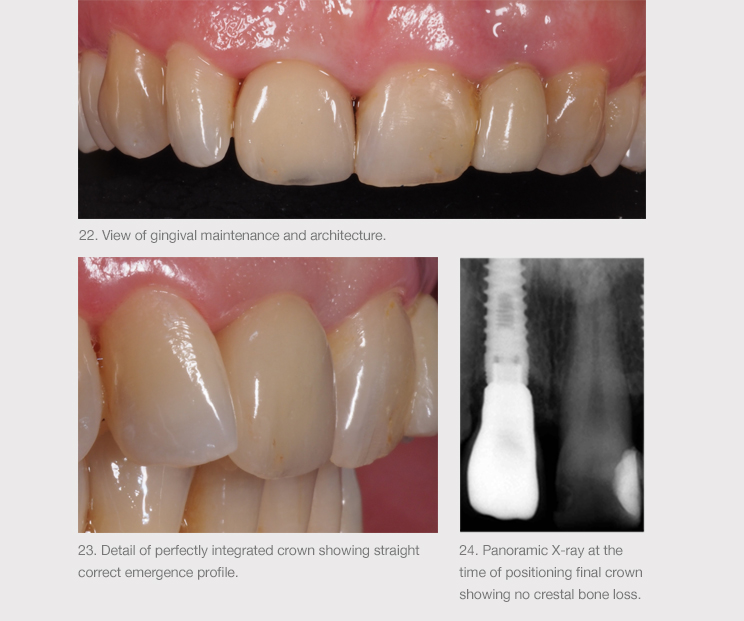
After 4 months, a personalized impression was taken by means of a customized flow closed tray transfer according to the emergence profile obtained with the provisional piece8, 9 and a final ceramic-metal crown screwed to the implant was created using CAD-CAM (Core3dcentres).


BIBLIOGRAPHY