



Hi! - ENG





The wide range of AVINENT prosthetic attachments allows us to perform optimal restorations, achieving a good functional and aesthetic result with an excellent level of patient satisfaction.
Case report
The patient is a 55-year-old woman, smoker, with no other medical history of interest and no known drug allergies, who consulted for failure of a fixed maxillary restoration.
The patient had a fixed prosthesis on upper 14 to 23 and on lower 47 to 43 and 33 to 35. Fracture of the upper stumps caused the front row to move and the prosthesis to fall continually. Two months previously, she had noticed a slight movement in the upper prosthesis, which made mastication impossible, interfered with her speech, and was becoming a problem in the performance of her daily tasks.
She also wanted to improve the appearance of the lower teeth and to prevent food from becoming lodged far back in the lower right quadrant.

 Baseline situation
Baseline situation
After confirming that all the remaining upper teeth were decapitated, and observing the presence of a ferrule of less than 2 mm and areas with subgingival cavities, we decided that it would be impossible to preserve the teeth. As for the lower teeth, we observed a cavity in the neck of 47, which caused the food impaction mentioned by the patient. We also observed gingival recession on all teeth, with exposure of the metal part of her fixed prosthesis.
The main complication in terms of prosthetics was the lack of space for vertical replacement of the teeth in the 1st and 4th quadrant, so we studied the possibility of levelling the bone in the upper arch and performing a restoration on the lower teeth using prosthetic materials that require little space.
A thorough clinical and radiographic study showed the presence of significant atrophy in the upper posterior quadrants. A residual alveolar ridge at the level of the maxillary sinuses prevented us from inserting implants in that area, and grafting was required. The CBCT confirmed the existence of bilateral intrasinusal bone septa in the area of the second premolar and first molar.
We drew up the following treatment plan:
Upper arch:
1. Bilateral sinus lift (SL)
2. Placement of 8 Biomimetic Ocean IC implants: 2 after SL healing, and 6 immediately post-extraction, with immediate loading of a temporary prosthesis. The implants located in the SL areas would not be loaded.
3. Zirconium-ceramic prosthesis with interface and dentures.
Lower arch:
1. Conservation of 42, 41, 31 and 32
2. Placement of implants in position 36 and 37
3. Zirconium crowns screwed on implants 36 and 37
4. Elevation of lower bridges
5. Extraction of the remnant of tooth 47
6. Reworking of the lower teeth to the existing gingival margin + placement of provisional acrylic teeth from 46 to 43 and from 33 to 35
7. Monolithic zirconia crowns with ceramic load in vestibular.
Procedure
Under local anaesthesia, the upper teeth were extracted and the Biomimetic Ocean implants (Avinent Implant System) were placed in the alveoli of teeth 11, 13, 14, 21, 23 and 25. In the area of 16 and 26 a double sinus lift was performed using a stratified technique, with 50% of autologous bone harvested from the maxillary tuberosity combined with bovine particulate xenograft, with delayed implant placement.
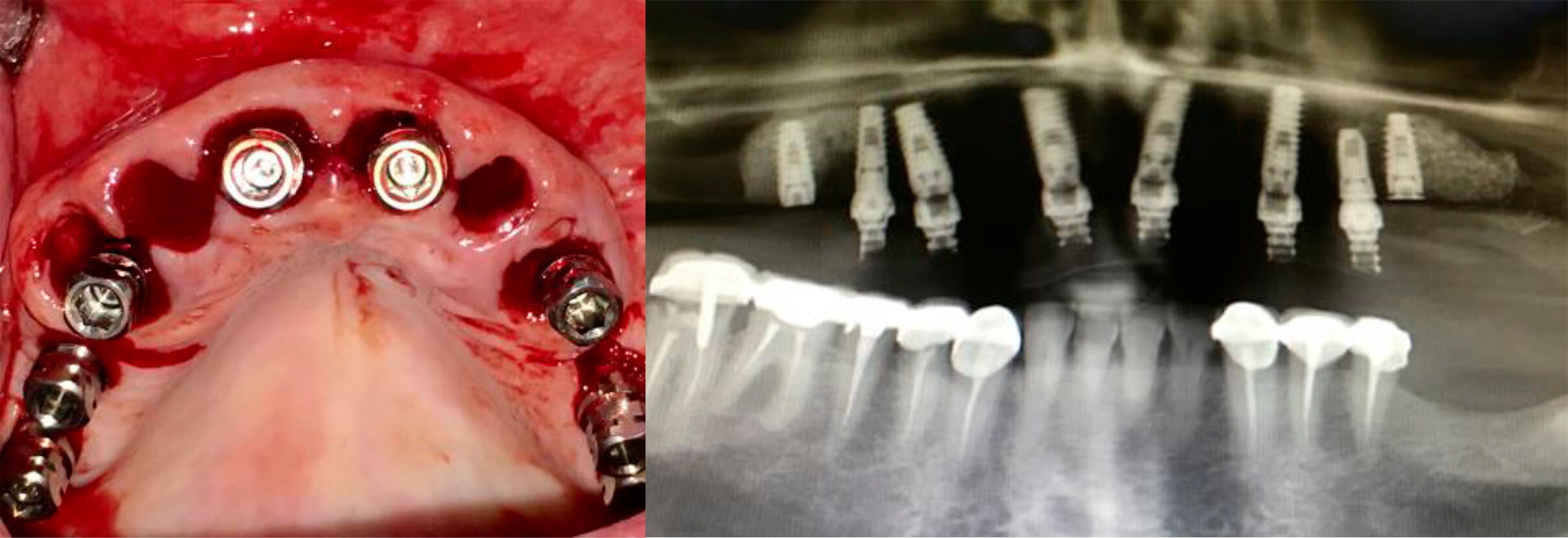 Post-extraction upper arch implants X-ray of implants and provisional prosthesis in place
Post-extraction upper arch implants X-ray of implants and provisional prosthesis in place
We achieved good implant stability, which allowed us to immediately load a temporary acrylic prosthesis from 14 to 25 with no distal cantilevers in order to avoid oblique or tangential forces that could negatively influence the osseointegration of the implants. The temporary prosthesis was planned and designed prior to surgery, and was placed 24 hours after the procedure.
Because we inserted transepithelial abutments of different heights on the implants, we were able to place temporary prosthesis-supported crowns, which allowed us to obtain optimal emergence profiles and maintain the anatomy of the papillae. This also achieved intrusion of the right occlusal plane in an attempt to obtain vertical space for the final prosthesis and as many occlusal contacts as possible.
In the lower arch, we placed a provisional PMMA prosthesis in order to evaluate gingival recession after remodelling. This prosthesis remained in place until complete osteointegration of the upper implants, and we were able to perform the final restoration of both arches simultaneously.
 View of the upper and lower immediate temporary prostheses
View of the upper and lower immediate temporary prostheses
 Detail of the temporary prostheses at 3 months
Detail of the temporary prostheses at 3 months
After placement of the upper implants, we waited 3 months before starting treatment on the lower arch in order to perform the final restoration of both arches at the same time, given the limited occlusal space available. In the upper arch, we chose a layered zirconia prosthesis to achieve the best aesthetic outcome.
In the lower arch, we placed a solid zirconia prosthesis with vestibular dentures to compensate for the lack of vertical space in the first and fourth quadrants. This gave a more satisfactory aesthetic outcome that more closely matched the colour of the patient’s lower incisors.
 X-ray of the definitive placement of the prothesis
X-ray of the definitive placement of the prothesis View of the definitive prosthesis in the mouth
View of the definitive prosthesis in the mouth View of the definitive prosthesis in the mouth
View of the definitive prosthesis in the mouth
Clinical outcome
Following the treatment, both the immediate post-extraction implants and those placed in the area of sinus lift were stable and fully integrated in the bone.
We managed to conserve the papillae and correct the upper right occlusal plane with inclusion, thus obtaining a more symmetrical smile and increasing the prosthodontic space between the first and fourth quadrants. This, in turn, gave the patient good occlusion, although the cusp of the right side was slightly flatter than that of the left due to the lack of space. We achieved correct canine-guided occlusion, with lateral protrusive disocclusion, despite the difficulty of the case. With respect to the lower arch, the implants in 36 and 37 were well integrated in the bone, and we achieved a major aesthetic improvement and stability of the gum at the level of the crowns after remodelling.
Conclusion
Avinent Biomimetic Ocean implants are particularly indicated for post-extraction treatments and immediate loading. Thanks to their conical design and active tip, the Ocean implant can be correctly placed in the alveolus, obtaining good insertion torques that permit immediate loading, and achieving an osseointegration rate similar to that of conventional deferred loading.
The wide range of AVINENT prosthetic attachments allows us to perform optimal restorations, achieving a good functional and aesthetic result with an excellent level of patient satisfaction.