



Hi! - ENG





Certain vertical defects in esthetic sectors can be corrected using prosthetic restorations without complex surgery or guided regeneration techniques.
INTRODUCTION
As described in the literature, the conventional treatment of cases where there is considerable vertical bone loss in the anterior sector can often lead to unsightly definitive restorations.
Proper planning using diagnostic imaging and diagnostic wax-up is essential in order to create the best treatment plan for the patient’s needs and to ensure a successful restoration.
As shown in this case, vertical defects of this type can be corrected through prosthetic restorations without the need to use guided regeneration techniques.
CASE DESCRIPTION
After suffering a serious injury to the anterior sector, with the consequent loss of bone and of soft tissue structure, the patient underwent several operations to stabilize and augment the alveolar ridge in the area. As the desired results were not achieved, a cemented prosthesis was used, but it did not meet the patient’s esthetic expectations.
As a result, some time later the patient came to the surgery seeking to have the esthetic appearance of his anterior teeth improved. The patient had a 1.2 to 2.2 cemented metal-ceramic prosthesis supported by the two side teeth, with two pontic teeth on the central incisors. The patient presented with considerable bone loss in sectors 1.1 and 2.1 due to the failure of two guided bone regeneration operations.
The patient also presented with inflammation and bleeding in the basal area of the pontic teeth and in the gum around the side teeth. The abutments showed a periodontal overload with widening of the ligament due to the disproportion of the teeth and an overload on the incisal guidance.
TREATMENT PLAN
The important psychological component of the case should be highlighted because the patient did not want to undergo any more operations due to the poor outcomes of the previous ones.
The proposal made to the patient involved the placement of two Biomimetic Coral IC implants (AVINENT Implant System) in positions 1.1 and 2.1, and subsequent restoration using individual cemented crowns. Treatment with a block bone and connective tissue graft to try to re-establish the alveolar and esthetic line was rejected. Instead, helped by a thick biotype and a low smile line, a restoration using artificial gum was performed.
CLINICAL CASE
Good planning is essential in order to create a proper treatment plan. This was not the case in this instance, because the patient arrived at the second stage of surgery without any type of study or planning being able to be conducted.

The implants were placed and a temporary acrylic bridge was positioned on the shaped teeth. At that moment in time, the prosthodontists ultimately saw the esthetic problem that this loss of tissue would have on the final prosthesis, which was exacerbated by the emergence of the implants in the vestibular area.


The proposed prosthetic solution consisted in placing two central customized metal-based zirconia abutments directly on the implant with artificial gum that would allow the insertion axis to be corrected. And four lithium disilicate crowns with a ceramic coating cemented on the shaped side teeth and on the abutments of the primary structure of the central teeth.
In cases like these, it is important to tell the patient about the esthetic limitations, due to the mimetic difficulties between the ceramic gum and the adjacent soft tissues. And about the need for rigorous routine hygiene in the basal area of the gum.
After accepting the treatment, and with the temporary bridge in place, work was done on the gingival contour on which the restoration would sit and, four months later, the definitive impressions were taken.
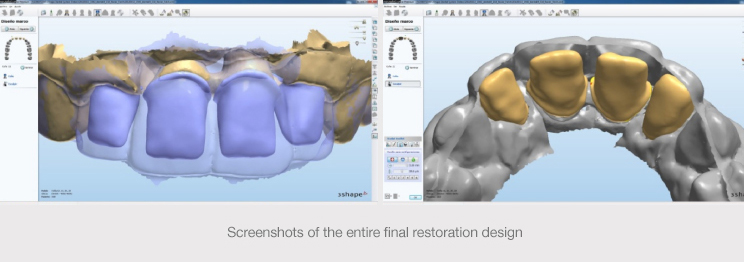
Due to the complexity of the case, a decision was taken to perform both a virtual wax-up and an analogue wax-up, with a digital version of the latter being created. The two files were superimposed, taking the analogue wax-up as the point of reference, in order to achieve greater precision in the structure.
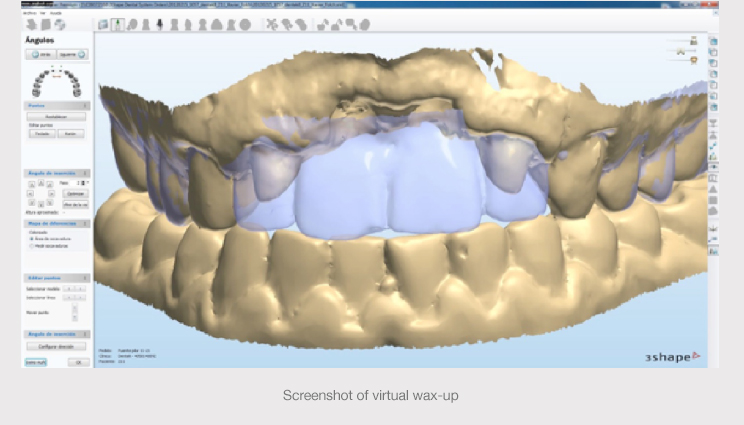
Based on the virtual wax-up, the primary zirconia structure formed by the central abutments and the base of the ceramic gum was designed, as were the lithium disilicate cores of the cemented crowns.
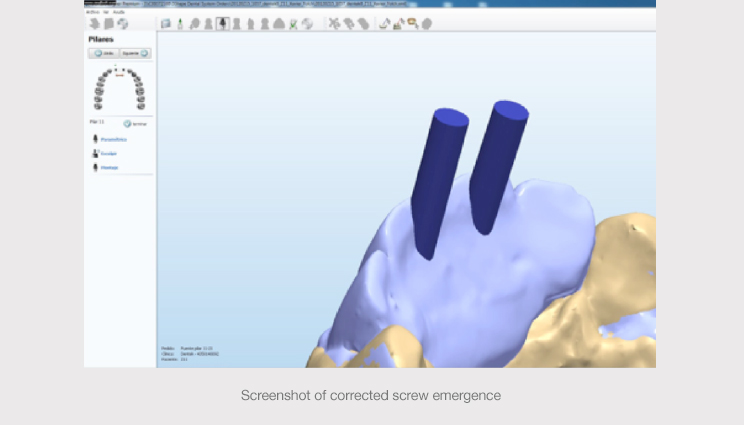
The software enabled the angulation of the abutments to be corrected, obtaining an emergence of the chimneys that, albeit not esthetic, allowed access to be optimized and the screws to be positioned in the palatal area without compromising the final work.
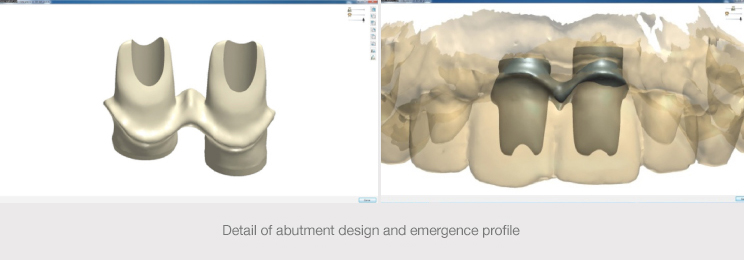
It also enabled the ceramic gum to be carefully incorporated into the structure, and to define the anatomy and emergence profile of the abutments, creating an optimum gum-tooth transition.
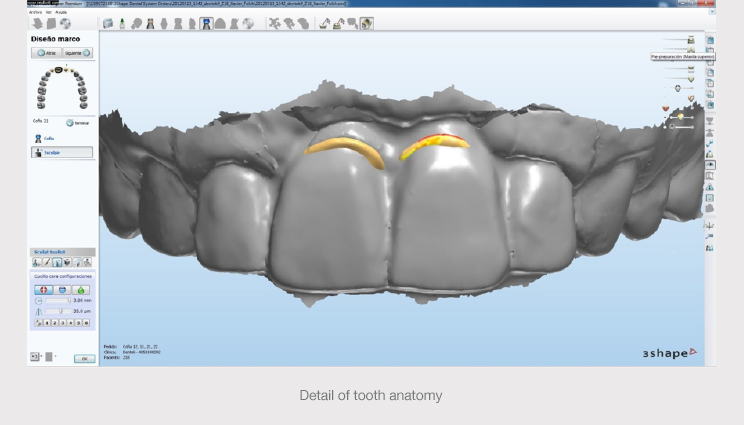
After pre-defining the primary structure, disilicate cores were designed, observing the structures separately and together, analyzing the critical points of the restoration at prosthetic, esthetic and functional levels.
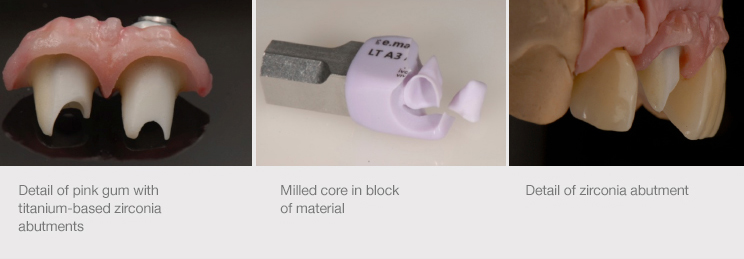
Finally, the primary zirconia structure was milled (AVINENT CAD CAM) and the titanium metal interfaces were cemented (AVINENT Implant System). The four lithium disilicate cores (e.max, Ivoclar) were also milled (AVINENT CAD CAM) and the crowns were made from coating ceramic (leucite-based e.max).
After checking the fit of the cores, the parts of the structure that would come into contact with the gum were polished and the artificial gum was made.
By means of photographic records, customized guides and tests on the patient, the clinical and technical team managed to achieve optimum integration of the tissues.
The metal bases were blasted following the adhesion protocol and the abutments were cemented.
The primary structure was screwed to the implants and the central abutments were sealed with interposing Teflon, whose composition was the same color as the zirconia.


The two central ones were cemented using temporary acrylic cement that would allow the crowns to be removed easily if required, and the side crowns were cemented using permanent cement.
The fit and the occlusion were also checked, and the patient was shown the hygiene protocol for the primary structure. The patient was very satisfied and an appointment was arranged to see the patient to re-assess the restoration after a fortnight. Having passed all the checks at one month and three months, an appointment was arranged to see the patient for the annual maintenance visit.


CONCLUSION
Certain vertical defects in esthetic sectors can be corrected using prosthetic restorations without complex surgery or guided regeneration techniques.
Through good planning, a good laboratory’s skill and the patient’s cooperation, this type of restorative dentistry solution with ceramic gum can solve the most complex cases in a highly satisfactory way for everyone involved.