



Hi! - ENG




With the appearance of intraoral scanners, soft tissue and teeth information (.stl) can be overlaid with high precision on the hard tissue information provided by CAT (DICOM).
Guided surgery has been used for many years with the aim of increasing precision in the placement of our implants. But its use has not extended to daily practice because of several disadvantages, primarily the cost of access and accuracy, given that CAT scan information had only been available until now for this procedure.
With the appearance of intraoral scanners, soft tissue and teeth information (.stl) can be overlaid with high precision on the hard tissue information provided by CAT (DICOM). This leads to significantly greater accuracy in surgery, especially in partially edentulous patients, because the surgical splints adapt perfectly to their position.
Surprise free operations can be undertaken by using a comprehensive 3D view plan of the surgery beforehand, having the information of all the tissues on which we will work and generating a guided surgery protocol with an exact surgical splint. The result is less morbidity, a reduction in the need to perform additional surgery (grafts, sinus elevation), fully guided prosthetic implants and, if required, the preparation of several high quality provisional implants.
CLINICAL CASE:
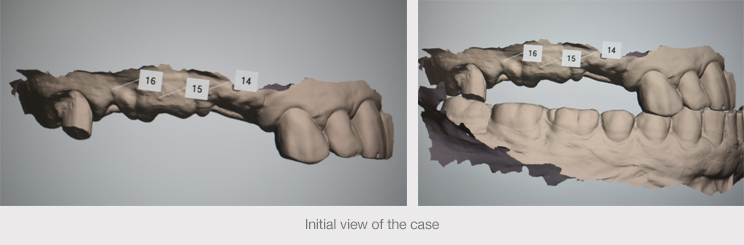
A 67-year-old male patient with controlled hypertension and similarly controlled type 2 diabetes, ASA III, visited the clinic because of the loosening of a tooth-supported fixed prosthesis positioned in the first quadrant from teeth 13 to 18, with an intermediate abutment in tooth 15
A clinical examination showed that both tooth 13 and 18 appeared viable and presented no signs or symptoms of endodontic leakage. Although tooth 18 had little ferrule and its prognosis in the medium-term was questionable, the decision was made to retain it. But tooth 15 appeared to be fractured and required extraction.
The choice of guided surgery was made in this case because of the patient’s baseline situation, the root angulation of tooth 13 and the proximity of the maxillary sinus, and there was no desire to perform grafts because of the first point.
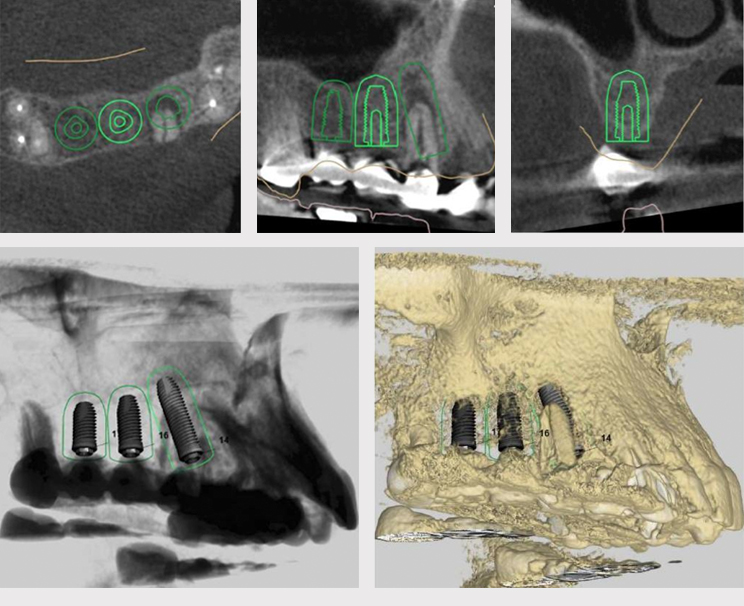
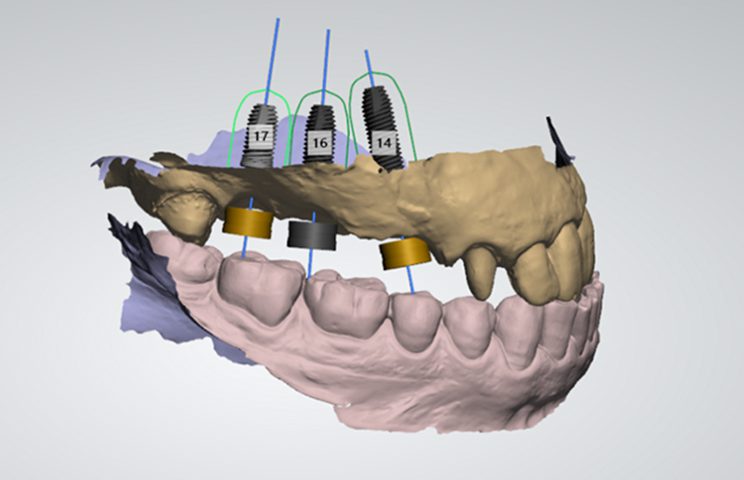
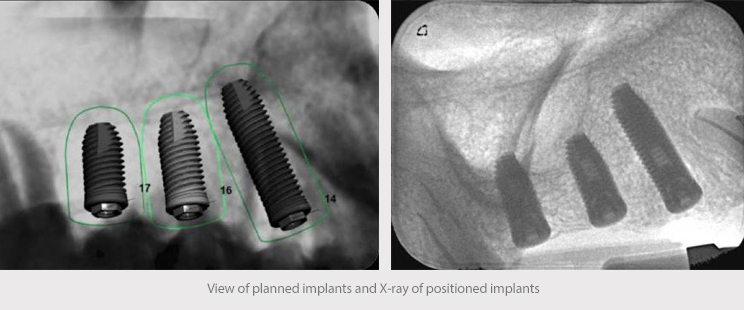
Avinent Coral IC implants were planned for all three cases. A 4.2 x 13 mm was placed in position 15 immediately after extraction and it was filled with xenograft, a 4.2 x 11.5 mm in 16 and, finally, a 4.2 x 10 mm in 17. The last implant was planned as a 4.2 x 8 mm and closed sinus elevation was performed with a 2 mm osteotome until positioning the 10 mm implant.
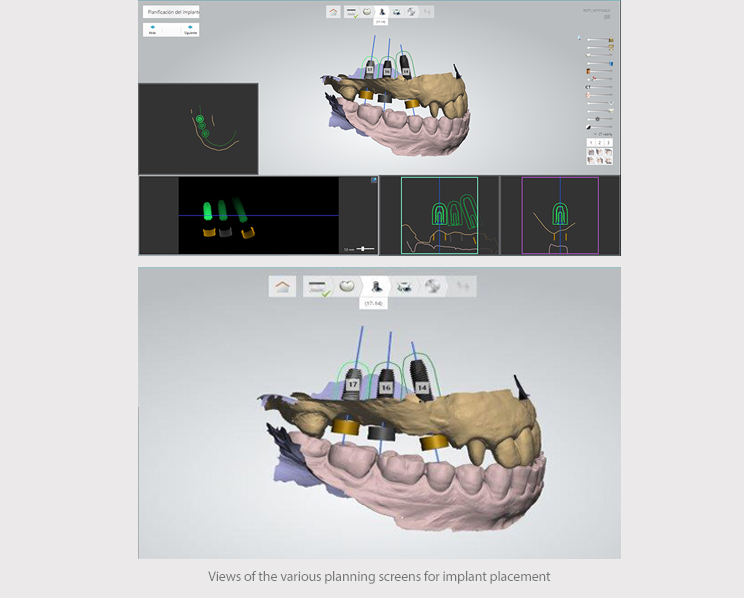
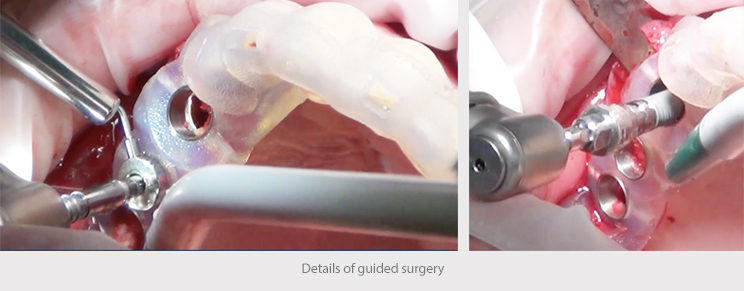
Open-flap surgery was used to position the implants, without any major detachment, according to the plan created by using Implant Studio (3Shape) software.
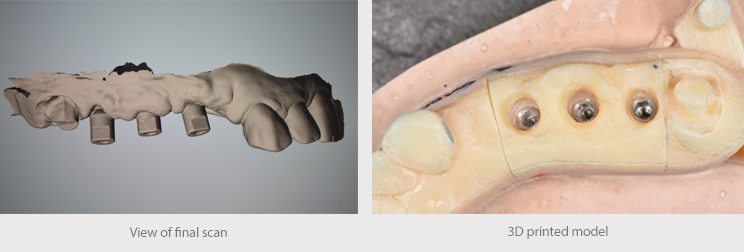
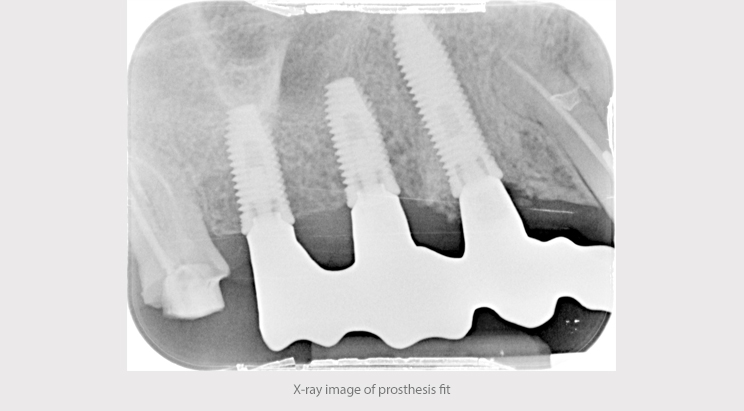
A second operation was performed after 12 weeks and prints were taken two weeks later with the TRIOS (3Shape) intraoral scanner to design the final restoration. A metal test of the chromium-cobalt milled structure was completed with angulation correction for tooth 15 and the ceramic was produced in the laboratory of Emilio Cuadrón Álvaro, placing a provisional PMMA in 18 and metal-ceramic crown with ceramic shoulder in 13.


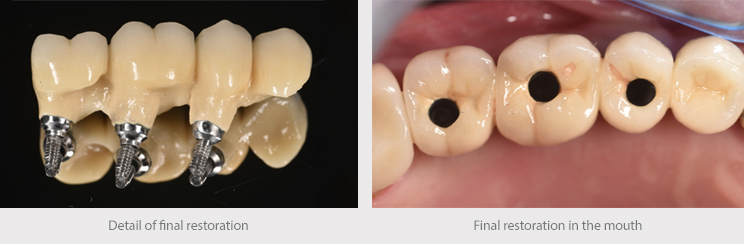
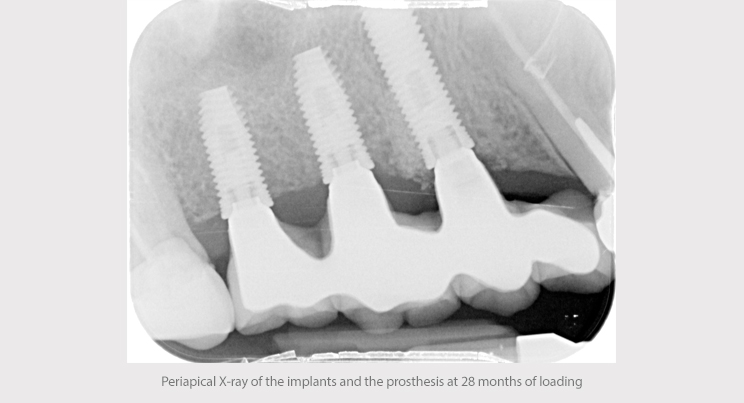
The extraction of tooth 18 was performed during the final revision, 28 months after the placement of the crowns on the implants. Otherwise, the functionality and gingival adaptation of the crowns on the implants remained intact without clinical or radiographic signs, or any peri-implantitis symptoms.
A simple, predictable surgical procedure could be undertaken thanks to suitable planning and guided surgery, with reduced morbidity in an ASA III patient, surprise-free restoration and a good long-term prognosis.